The Integrated OR: What Video Routing, Documentation and Device Control Actually Buy You
15 June 2026 · By Medtech
Every hospital director eventually sits through the integrated OR pitch: screens everywhere, a touch panel, a rendering of the theatre of the future. The pitch is easy to admire and hard to evaluate. What does integration actually buy you, in workflow, in documentation, in clinical capability? And which parts can safely wait for a later budget cycle?
We design and install OR integration as part of our theatre solutions work, in the context of the Karl Storz integration ecosystem, alongside the Zeiss microsurgery optics and Draeger theatre infrastructure we supply. Here is the honest version of the value case.
What integration actually is
Strip away the showroom and OR integration is three functions:
- Video routing: any image source in the theatre, endoscopic camera, room camera, surgical microscope, imaging viewer, delivered to any display, in the right format, without anyone re-plugging cables mid-case.
- Documentation and data management: capture of stills and video against the correct patient record, stored securely, retrievable and exportable when needed.
- Device control: core theatre devices, camera, insufflator, light source, room lighting, operated from a central interface usable from the sterile field, rather than five separate front panels around the room.
Everything else in the brochure, streaming to a seminar room, video conferencing, dashboards, builds on those three foundations.
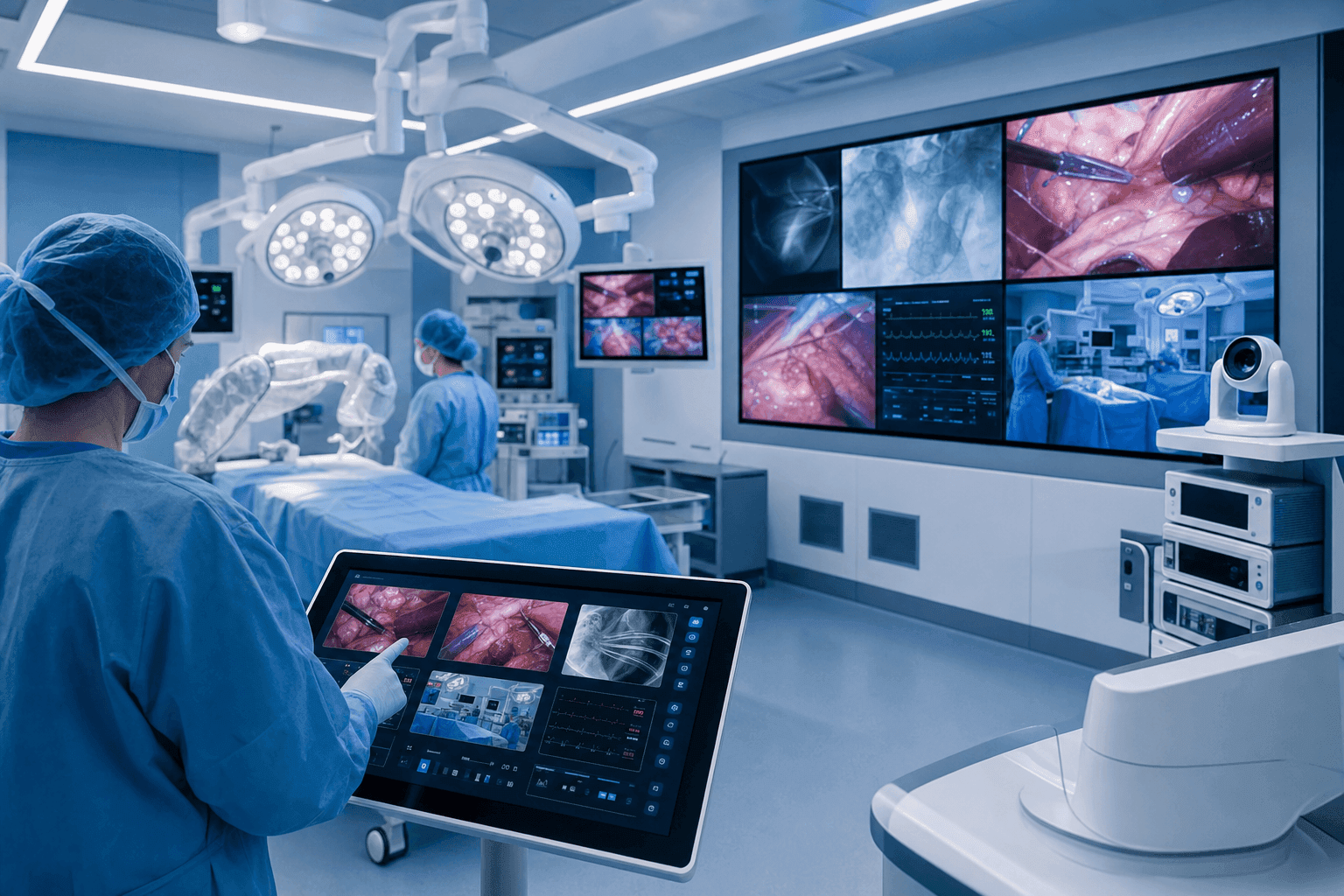
Video routing: the right image, at the right screen, now
The clinical value is simple: everyone sees what they need without breaking scrub or craning past a colleague. The surgeon operates facing a well placed monitor instead of twisting toward a tower. The scrub nurse anticipates because the field is visible from her position. The anaesthetist watches the laparoscopic view during the moments that matter. Fewer cables cross the floor, which means fewer trip hazards and faster room turnover between cases.
Routing quality lives in details that are invisible at demonstration stage: latency, resolution preserved end-to-end, and predictable behaviour when a source drops. Specify the whole chain, because the weakest component sets the image quality for the entire room.
Optics still decide what there is to route
Integration distributes images; it cannot improve them. The camera head, the endoscope and the microscope decide what everyone sees on those elegant displays. This is why we treat integration and imaging as one procurement conversation: Karl Storz camera platforms and endoscopes on the minimally invasive side, and Zeiss optics where microsurgery demands them, in neurosurgery, ophthalmology and spine. A theatre that upgrades its routing while running tired scopes has decorated its weakest link.
Documentation: the quiet business case
Documentation is the least glamorous function and often the strongest justification. When capture is integrated, images and video attach to the correct patient automatically, as part of the case rather than as an extra chore competing with patient care. The value compounds across the hospital:
- Medico-legal defensibility: a contemporaneous visual record of what was found and what was done.
- Referral quality: letters that carry images rather than descriptions of images.
- Training: a growing library of real cases for junior staff, built passively.
- Audit and morbidity meetings reviewed from footage rather than from memory.
Governance must be specified at design stage, not patched afterwards: retention periods, access control and export rules all belong in the project definition.
Device control and workflow
Central control sounds like a luxury until you count interruptions. Every adjustment that pulls the circulating nurse to a different front panel, every settings hunt between cases, is a small delay multiplied across a full list. Integrated theatres use presets: the room configures itself for a laparoscopic list, a specific surgeon, a specific procedure, in moments. Units running integrated theatres report smoother turnover and fewer intraoperative interruptions, and the consistency itself has value, because a room that is always set up the same way is a room where errors are easier to see.
We deliberately avoid promising specific minutes saved. Published experience varies with case mix and baseline discipline. The direction of the workflow gain, however, is consistent.
A phased upgrade model
A full integration project in one step suits a new build. Existing theatres usually phase the journey, and phasing works well:
Phase 1: the imaging chain
Modern camera platform, endoscopy and displays. Immediate clinical benefit, no structural work, and every later phase inherits the image quality.
Phase 2: routing and documentation
Video management plus capture linked to patient records. Ceiling booms and additional displays where the building allows. This is where the workflow and medico-legal gains land.
Phase 3: full integration
Device control, room presets, streaming and conferencing, and integration of the microscope and room systems into one environment. This stage also positions the theatre for what comes next: robotic and computer-assisted surgery assume an integrated video and data environment as their foundation. We explore that frontier in depth at robotic.mu.
Each phase stands on its own operationally and financially, budgets stay predictable, and the theatre is never out of service for long stretches.
Planning the project
Integration succeeds or fails at the site survey: structural checks for boom loads, electrical and network capacity, and honest workflow interviews with the people who run the lists. Installation is scheduled around your operating calendar, staff are trained by role, and our clinical support team stands in theatre for the first integrated lists, the same support model we run across our surgical portfolio. Our Operating Room portfolio covers integration alongside surgical lights, tables, sterilization and the imaging chain itself.
If a theatre upgrade is on your capital agenda, involve us at feasibility stage. The earlier the conversation, the cheaper the good decisions. Start it through our contact page.
Over 30 years advancing healthcare in Mauritius, Seychelles and Madagascar. Explore the wider Chemtech Group health ecosystem.