Cemented vs Uncemented Hip Arthroplasty: Selecting Systems for an Ageing Island Population
12 June 2026 · By Medtech
The hip arthroplasty conversation in Mauritius is changing. An ageing population means more elective hips in patients over seventy, more fragility fractures of the femoral neck, and more revisions arriving a decade after the first wave of primaries. Each of those trends pushes on the same old question: cemented or uncemented fixation?
There is no universal answer, and any supplier who offers one is selling rather than advising. What follows is the framework we discuss with orthopaedic teams, grounded in the Medacta hip portfolio we supply and support in theatre.
Two philosophies of fixation
Cemented fixation secures the implant with bone cement that interdigitates with the prepared bone surface. Stability is immediate and does not depend on the bone's capacity to grow. That makes cement forgiving in osteoporotic, capacious femoral canals, which is exactly the bone that ageing produces.
Uncemented fixation relies on a press-fit implant with a surface engineered to encourage bone to grow onto or into it. It depends on solid initial mechanical stability and on bone that is biologically able to respond. In the right femur it produces a durable biological bond with no cement mantle to manage.
Neither philosophy wins everywhere. The task is matching fixation to the bone and the patient in front of you.
What the registry evidence suggests
National joint registries have followed very large cohorts of hips for decades, and their signal is consistent in direction even where the details differ between countries:
- In the oldest patient groups, cemented stems are associated with fewer early periprosthetic fractures and fewer early revisions than uncemented stems.
- In younger patients with good bone stock, modern uncemented systems perform well over long horizons.
- For hemiarthroplasty after femoral neck fracture, published guidance in several health systems favours cemented stems for the typical elderly fracture patient.
We cite the direction of this evidence rather than specific figures deliberately. Registry numbers shift with every annual report, and the fixation decision belongs to the treating surgeon. The pattern, though, is stable enough to plan a service around: an ageing island population means cementing skills and cemented inventory are becoming more important, not less.
Reading the bone, not the birthday
Age is a proxy, not a rule. The practical assessment happens on the radiograph and in the canal:
- Canal shape. The classic classifications distinguish narrow, funnel-shaped canals with thick cortices from wide, stovepipe canals with thin cortices. Wide, thin-walled canals argue for cement.
- Bone quality. Osteoporosis, long-term steroid use, renal bone disease and inflammatory arthropathy all weaken the case for press-fit fixation.
- Clinical context. An elective osteoarthritic hip in a fit sixty year old and a displaced femoral neck fracture in a frail eighty five year old are different operations with different fixation logic, even where the implant catalogue overlaps.
- The team's pathway. Cementing is a discipline of its own: canal preparation, cement timing, pressurisation and venting. A department that cements rarely should train before it needs the skill on an emergency list, not during it.
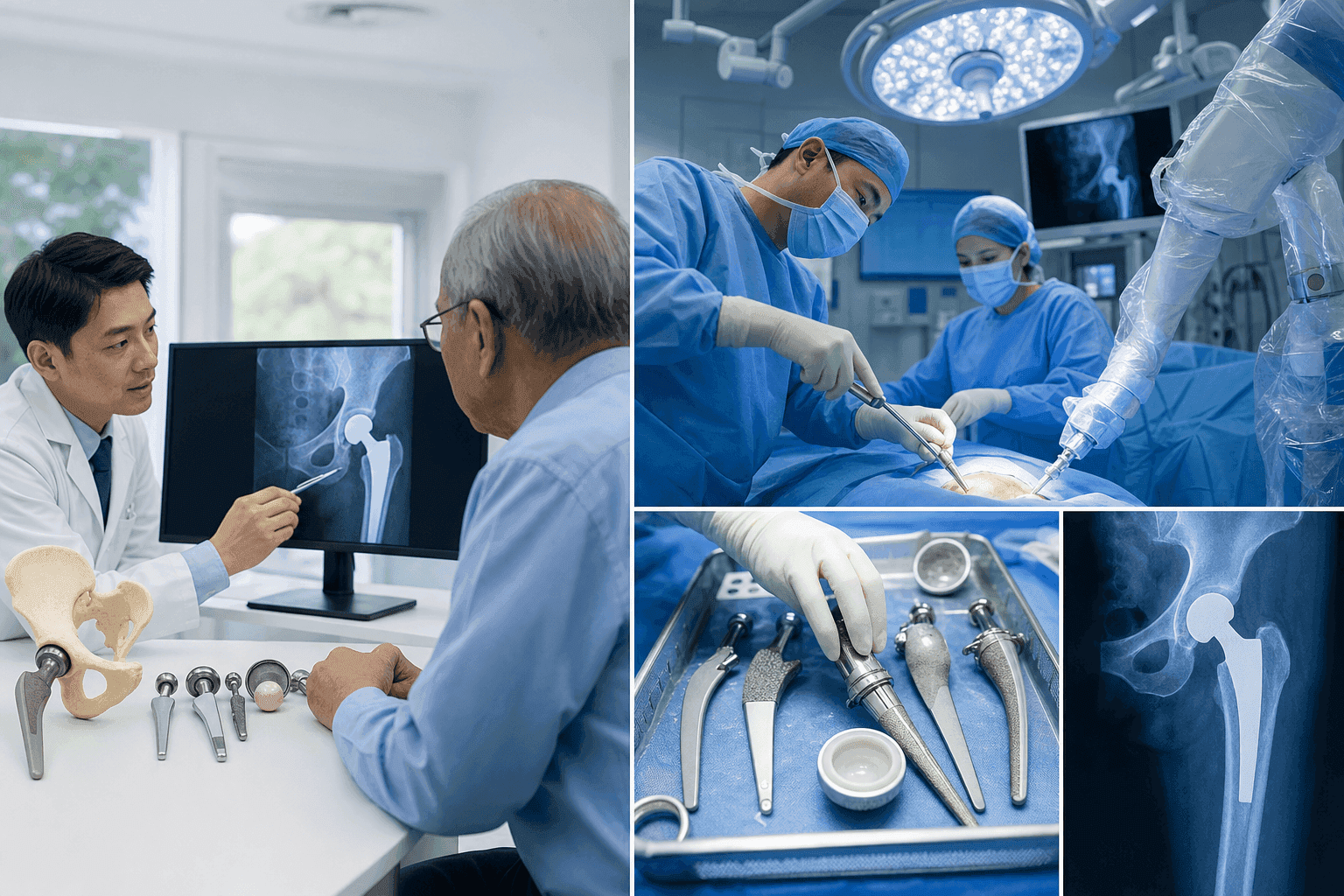
The MectaCem line and the revision horizon
We supply the Medacta MectaCem cemented hip system alongside uncemented options, bipolar heads for fracture hemiarthroplasty, and revision implants for the cases that come back years later. That breadth matters for one practical reason: a hospital should not have to change supplier mid-pathway. The partner that supports your elective primaries should also be able to support your fracture service and your revisions, with compatible instrumentation and a technical team that knows all three workflows.
What a complete implant service includes
An implant system is only as good as the logistics behind it. When we take on an arthroplasty service, the package looks like this.
Consignment sets on site
Full size runs of implants and instrumentation held at the hospital on consignment. You pay for what is implanted; we monitor and replenish the stock. For fracture work, where the next case cannot wait for a courier, consignment is not a convenience. It is a patient safety measure.
Instrumentation and sterilisation logistics
Complete, maintained instrument trays with a defined turnaround, so back-to-back lists do not stall on processing, and worn instruments are replaced before they become an intraoperative surprise.
In-theatre technical support
Our product specialists attend cases on request, particularly first cases on a new system, complex primaries and revisions. Sizing and instrumentation questions get answered at the table, not after it. This is the in-theatre support model we run across our surgical portfolio, staffed by nurses, biomedical engineers and technicians.
Training and CPD
Surgeon-to-surgeon education through the manufacturer network, plus structured training for theatre and sterile services staff through our learning platform and CPD sessions with local accredited providers.
Planning for an ageing decade
If your service expects the demographic curve the whole region expects, the planning conclusions are straightforward:
- Run a genuine dual-fixation service, with modern cemented and uncemented systems both on the shelf and both rehearsed.
- Audit your cementing technique and refresh it formally before fracture volumes force the issue.
- Put fracture hemiarthroplasty inventory, including bipolar heads, on consignment so emergency lists never wait on logistics.
- Agree the revision pathway with your supplier now, while it is hypothetical, rather than during the first difficult case.
Our full Orthopedic portfolio covers hip and knee arthroplasty, spine, trauma and sports medicine, with the same consignment, training and in-theatre support model behind every line.
If you are reviewing your arthroplasty supply arrangements or building a fracture pathway, talk to us through the contact page and we will walk the options through with your team.
Over 30 years advancing healthcare in Mauritius, Seychelles and Madagascar. Explore the wider Chemtech Group health ecosystem.