Building a Dialysis Unit in Mauritius: From Reverse Osmosis Water to Chronic Therapy Protocols
13 June 2026 · By Medtech
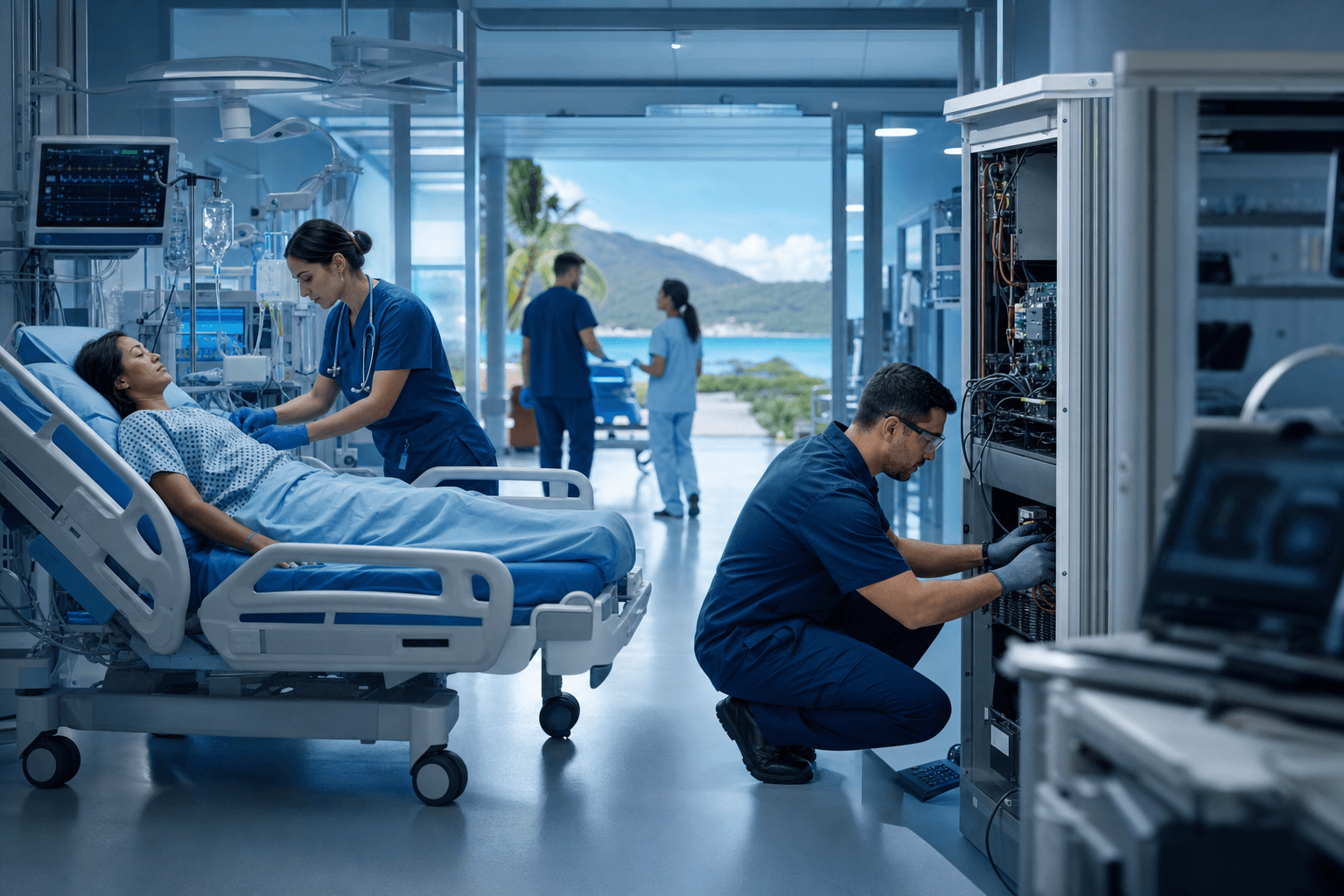
Demand for dialysis in Mauritius continues to grow, driven by the island's well documented burden of diabetes and hypertension. For clinic owners and nephrology leads, that demand translates into a hard planning question: what does it actually take to open a dialysis unit, and to run it safely for patients who will depend on it several times a week, for years?
We supply and support the Fresenius Medical Care dialysis portfolio in Mauritius, from reverse osmosis water plants through machines to consumables. This guide sets out the planning sequence we walk through with every new unit.
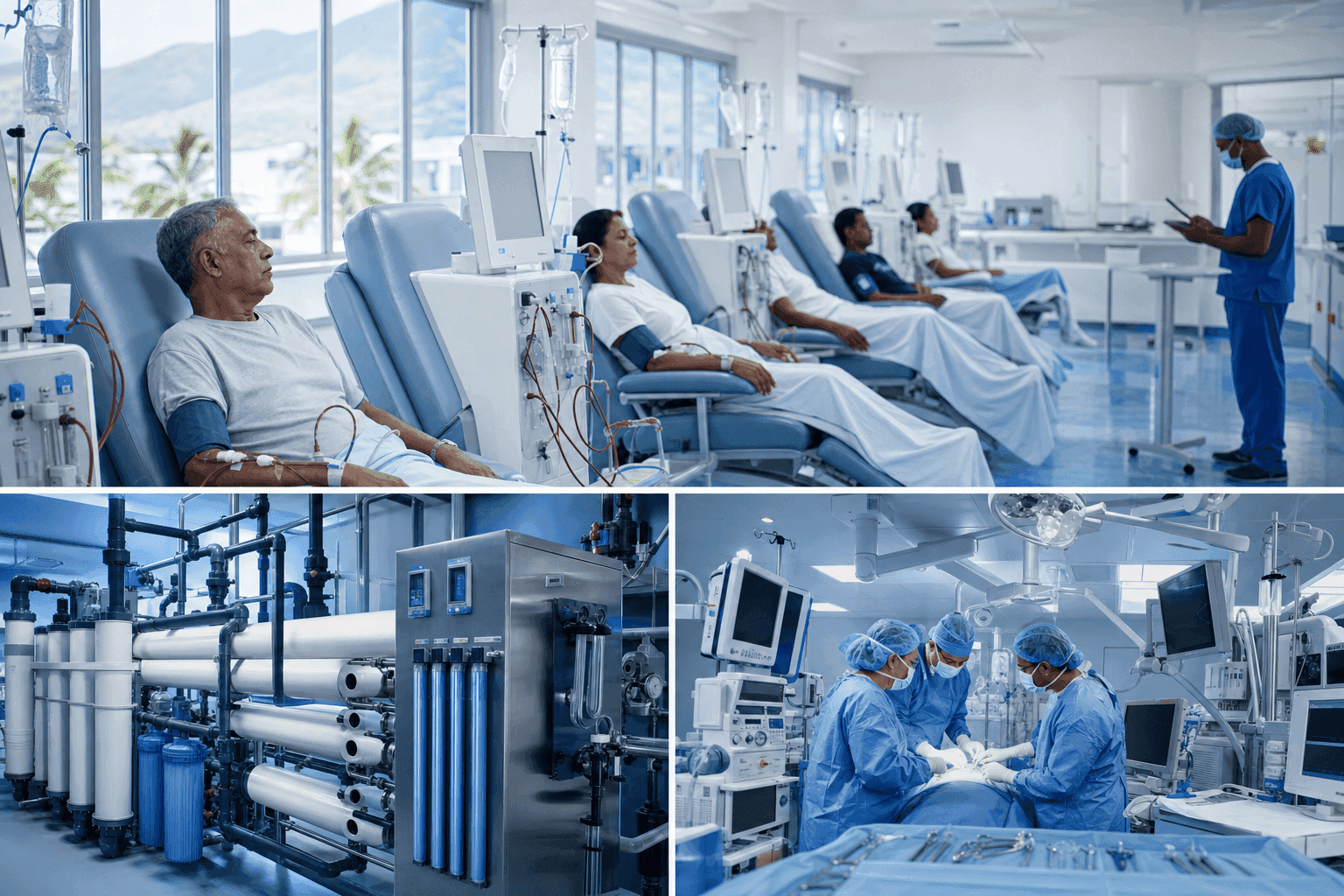
Start with water, because everything else does
Every haemodialysis session brings a patient's blood into indirect contact with a volume of treated water far beyond anything the rest of medicine asks of a supply. Water quality is therefore not a facilities detail. It is a clinical parameter, and it is designed in or designed out at the construction stage.
A dialysis water system has four layers:
- Pretreatment: sediment filtration, softening and carbon filtration matched to the municipal feed water, which varies by region of the island and by season.
- Reverse osmosis: the RO plant itself, sized for peak simultaneous demand, ideally with redundancy so a membrane failure does not close the unit for a week.
- Distribution: a circulating loop, designed without dead legs, that keeps treated water moving to every station.
- Disinfection and monitoring: a scheduled regime of chemical or heat disinfection, plus routine microbiological and endotoxin testing against the international standards for dialysis water quality, the ISO 23500 series.
Decisions taken here, loop layout, sampling ports, redundancy, determine your infection control workload for the next fifteen years. We size and install RO plants as part of unit design, never as an afterthought to a machine order.
Sizing the machine fleet
Fleet sizing is simple arithmetic plus honesty about growth:
- Fix your treatment schedule first: how many shifts per day, how many days per week.
- Each station treats one patient per shift, so stations multiplied by shifts and days gives weekly capacity.
- Hold back margin. Machines need preventive maintenance windows, and a fleet with zero spare capacity turns every technical fault into a cancelled treatment.
- Plan the growth curve. Chronic programmes rarely shrink. Water loop take-offs, power points and floor space for future stations cost little during construction and a great deal afterwards.
We help units model these choices against the Fresenius machine range, including whether to specify haemodiafiltration capability, which affects both water demand and consumable logistics.
Consumables: the logistics tail that wags the dog
A dialysis unit consumes stock relentlessly: dialyzers, bloodlines, fistula needles, concentrates and disinfectants, per patient, per session, indefinitely. On an island, the buffer stock question is existential. A delayed container must never translate into a missed treatment.
Our answer is the consignment model we run across our portfolio: agreed stock held at your unit, monitored and replenished by us, paid for as it is used. Combined with scheduled import cycles managed by our Import and Export team, it gives a unit a defined number of weeks of autonomy, agreed in advance, rather than an improvised cupboard count. The same team handles export logistics and customs compliance for units in Seychelles and Madagascar.
Acute and chronic are different services
The same unit often serves two populations with very different logic:
- Chronic therapy is scheduled, capacity-driven and protocol-stable. Success is measured in dialysis adequacy, vascular access care and uneventful years.
- Acute therapy is unscheduled and clinically volatile: acute kidney injury, intensive care support, patients too unstable for a standard chronic slot. It may need dedicated machines, portable RO capability for bedside treatments, and staff trained for a different rhythm.
If your business plan includes hospital support contracts, specify the acute capability from day one, covering machine features, water portability and staffing, rather than improvising it after the first urgent referral arrives.
Protocols, people and paper
The technology is necessary but not sufficient. Before first patients, a unit needs:
- Water quality logs and a testing calendar aligned to the standards above
- Machine disinfection protocols between patients and at end of day
- A preventive maintenance contract with defined response times, backed by locally held spares; our Technical Excellence team is based in Mauritius and factory trained on the platforms we install
- Staff training: we train nurses and technicians on the equipment we supply, through hands-on sessions, our learning platform and CPD with local accredited providers
- A quality framework for documentation and traceability; our own operations are certified to ISO 9001:2015, and we align our supplier documentation to your accreditation needs
One partner from slab to first session
The units that open smoothly are the ones where water, machines, consumables and training were planned as a single system rather than four separate purchases. Our Renal Support portfolio spans reverse osmosis, chronic and acute dialysis therapy and consumables, with installation and maintenance handled by the same local team. For a deeper dive into therapy options and unit planning, our dedicated renal resource at dialysis.mu continues this series.
Planning a new unit, expanding an existing one, or rethinking an ageing water plant? Talk to our renal team through the contact page and we will help you sequence the project from slab to first session.
Over 30 years advancing healthcare in Mauritius, Seychelles and Madagascar. Explore the wider Chemtech Group health ecosystem.